

Abstract
Background
Acute pulmonary embolism (PE) is the leading cause of maternal mortality in Western countries, accounting for 20 to 30% of all maternal deaths. Therefore, the threshold to test for PE during pregnancy is low. Because evidence regarding the safety of ruling out PE with clinical decision rules and D-dimer tests in pregnant women is unavailable, all women with a suspected PE need to undergo an imaging test, with potential harm to patient and fetus by exposure to ionizing radiation. In the present international, multicenter, prospective management study, we evaluated the safety and efficiency of the YEARS diagnostic algorithm for ruling out PE in pregnant patients with clinically suspected PE (Netherlands Trial Registry number 5913). YEARS is a simple diagnostic algorithm designed to reduce the number of required computed tomography (CT) scans in the diagnostic work-up of PE in non-pregnant patients, and was recently shown to be as safe as conventional algorithms but associated with a significant absolute 14% reduction in the number of CT scans (van der Hulle et al., Lancet 2017).
Methods
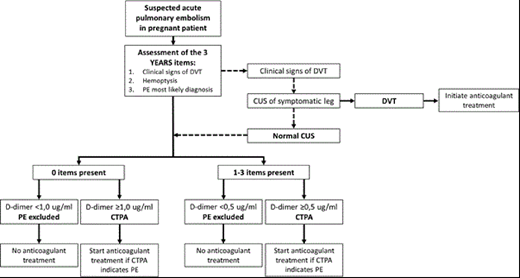
The Artemis study was performed in 11 Dutch hospitals, 8 French hospitals and 1 Irish hospital. Consecutive pregnant patients with suspected acute PE were included. Exclusion criteria were treatment with therapeutically dosed anticoagulants >24 hours or contraindications for CT. The YEARS algorithm was slightly adjusted for application during pregnancy (figure 1): in patients with signs of deep vein thrombosis (DVT), compression ultrasonography was obligatory before CT scanning was considered. In patients with proven DVT, anticoagulant treatment was initiated and no further diagnostic tests were undertaken. In patients with no YEARS items (Figure 1), a D-dimer threshold of <1.0 µg/ml was sufficient to rule out PE. In the remaining patients D-dimer threshold was <0.5 µg/mL. CT scanning was only performed in patients with a D-dimer level above the threshold. Anticoagulant therapy was withheld if PE was excluded. The primary safety endpoint was the occurrence of symptomatic venous thromboembolism during 3 months of follow-up, the primary efficiency endpoint was the proportion of patients in whom CTPA could be avoided. All safety endpoints were adjudicated by an independent committee. Assuming a 1.0% diagnostic failure rate and defining a maximum acceptable failure rate of 2.7%, a total study population of 472 patients was required (one-sided alpha 0.05, beta 80%).
Results and conclusion:
The last patient was included in May 2018. At baseline, 48% of pregnant women with suspected acute PE had no YEARS item and a D-dimer threshold of 1.0 µg/mL was applied. A total of 42% had a D-dimer level below the relevant threshold and were managed without CT scanning. Follow-up and endpoint adjudication was not completed at the abstract submission deadline; full study results will be presented at the ASH meeting.
Couturaud:Pfizer: Research Funding; Bayer: Honoraria, Other: Travel Support; AstraZeneca: Honoraria; Actelion: Other: Travel Support; Intermune: Other: Travel Support; Leo Pharma: Other: Travel Support; Daiichi Sankyo: Other: Travel Support.

